
You may have heard about ultrasound used as a post-rehabilitation technique after surgery or perhaps you’ve used a heating pad to ease back pain. There are many techniques involving the application of heat, which are purported to treat a variety of symptoms. In this post, I’ll briefly cover the categories of techniques, common physiological effects of thermotherapy according to the literature, and the treatments it could potentially benefit and end by summarizing findings of the research included. As always, sources used for this post are referenced at the end.
—-
Thermotherapy is defined as the application of a modality with a higher temperature than body temperature to induce changes in tissues, but is the heating of tissues enough to really make therapeutic changes? As usual, the answer depends on the modality and the outcome goals of treatment.
There are two categories of thermotherapy: Superficial and deep.
Superficial thermotherapy is the application of heat to superficial tissues with a depth of penetration equal or less than 1cm. If you think about how big 1cm is you can imagine the problem with this technique for treating things like muscles and deeper tissues. Will a superficial hot pack actually reach a muscle underneath it? Perhaps, if you are heating a hand muscle, or an area of thin skin where the muscle is more superficial, but it’s unlikely that you will have much success reaching deeper tissues with superficial heat using such items as hot packs, and whirlpools. While in certain areas of the body the penetration can be deeper than 1cm, it is not likely to offer therapeutic benefits. Again, this does depend on what you are trying to do therapeutically. To induce mild inflammation (remember, acute inflammation is a good thing) or accelerate metabolic rate, a temperature increase of 1.8 degrees Fahrenheit is necessary. To decrease muscle spasm, reduce pain or increase blood flow, a heat increase of 3.6-5.4 degrees Fahrenheit is necessary. For superficial heat, a hot pack or a whirlpool are referenced by most studies as falling short of a 3.6 degrees Fahrenheit temperature increase on muscles such as the triceps surae and the quadriceps and the depth of penetration is very shallow. If you want to heat up the joint capsule of a shoulder, a hot pack will never be sufficient because it is too deep in body. A modality has to penetrate deeply enough to reach the area needing treatment.
Another modality for superficial heat is a hydrocollator. A hydrocollator is a moist-heat pack that has a typical temperature of 160-170 degrees Fahrenheit, and when applied to quadriceps for 20 minutes, can increase temperature at 1cm depth 6.5 degrees F and at 3cm depth, 1.4 degrees F. These heat packs are so hot they must be applied with a covering pad.
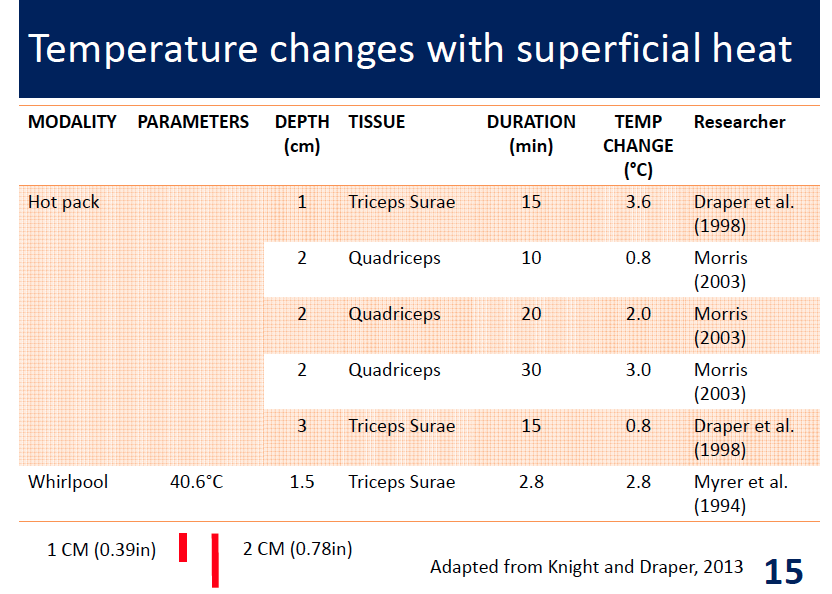
This photo above is from a slide borrowed from my professor summarizing research on depth of penetration and duration of application and their combined effect on temperature increase in the referenced tissues.
Deep thermotherapy is the application of heat modalities, which cause tissue temperatures to rise in deeper tissues (typically 3-4cm). We will focus on ultrasound since it is a common treatment modality in deep thermotherapy. Ultrasound is an acoustic mechanical agent using acoustic vibration to produce heat as a byproduct. Electrical energy is converted to acoustic energy within the sound head of the device and is typically conducted through a water-based gel substance to the body. High frequencies (3MHz) have a high absorption rate and low penetration depth (less than 3cm) and are best for superficial tissues. For superficial tissues, a treatment time of 3-4 minutes is typical though these depend on size of treatment area, intensity etc. Lower frequencies (1MHz) can penetrate deeper (5-7cm), but with less absorption. Clinicians should consider which frequencies to use depending on the treatment area depth. For lower frequencies, 10-12 minutes is therapeutically typical, but depends on various factors surrounding the treatment. A 1MHz frequency might be best for a rotator cuff or the vastus intermedius muscle, whereas the 3MHz output might be better on a patella tendon, MCL or the brachialis muscle. In addition to frequency settings, there is also continuous (100% duty cycle) or pulsed-wave output (chosen by therapist). Pulsed ultrasound has been found effective to decrease pain and increase range of motion as well as accelerating fracture repair. With both modes of ultrasound therapy, there are both thermal and non-thermal effects.
Physiological Effects of Thermotherapy:
As you read the physiological effects of heat below, keep in mind the depth of the various tissues being discussed and the type of modality used and think about whether this treatment could even reach these depths and induce necessary changes in temperature to a therapeutic value. If you are not interested in the physiological effects, just skip down to the “Clinical Applications” section.
Circulation & Fluid Dynamics of Heating:
Applying heat can increase blood flow circulation 1-2 times beyond normal flow and can increase cell metabolism. The increase in cell metabolism can be beneficial during the healing process, but is devastating immediately following an injury because it can induce secondary metabolic injuries in surrounding tissues by increasing the demand for oxygen and increasing waste products. Heat can also increase edema, especially in non-elevated limbs so it is important to not use heat early in an injury. If heating must be used while there is edema, the limb should be elevated. Heat will dilate superficial blood vessels causing relaxation of smooth muscle walls (most vessels have smooth muscle walls). Heat can decrease blood viscosity (thickness), which also increases the rate of flow. Heat is pro-inflammatory and will increase delivery of leukocytes to the heated area. While the inflammatory process is important for healing after an injury, the negative effects of heating early in an injury outweigh the benefits. This is why it’s important to consider the entire picture of injury healing and not focus only on one factor as if it is a separate entity.
Nerve Conduction effects from heating (aka Pain reduction):
Heat is often used to reduce pain and it has both a direct and indirect mechanism for doing so. The direct effect is to increase the pain threshold by increasing the conduction velocity of nerves that can transmit pain information. Indirectly, heat can lessen the mechanical pressure by reducing edema and decreasing muscle spasms, which then can reduce pain. Muscle spasms are reduced by decreasing gamma-motoneuron sensitivity, increasing blood flow, and reducing local muscle metabolites.
Tissue Elasticity effects from heat:
An increase in tissue temperature of 5-7 degrees Fahrenheit for 5 minutes is sufficient to increase tissue extensibility. To achieve plastic deformation, the tissue should be heated to 104-113 degrees Fahrenheit and to deform the tissues, stretching is required during or immediately after heating. Therapeutic temperature ranges of heat are higher than we think and this can be painful or uncomfortable for some people to tolerate.
Proposed Non-thermal effects of ultrasound:
It has been proposed that non-thermal effects of ultrasound can also be beneficial if began 72 hours after injury. Benefits may include: increased calcium ion influx through increased histamine release, increased capillary density in ischemic tissues, increased fibroblastic activity, attraction of immune cells to the area, increased collagen deposition, decreased edema (by liquefying the viscosity), accelerated fracture repair, and formation of stronger collagen tissue.
Clinical Applications:
Both thermal and non-thermal effects can occur in continuous and pulse wave ultrasound treatments and the thermal effects are generally enhanced when the duty cycle approaches 100%. The size of the treatment area should be 2-3 times the size of the sound head and if the area is larger, it should be split into two different sessions. Absorption of ultrasound heat is highest in tendons, ligaments, fascia, joint capsules and scar tissue and has been found effective at accelerating fracture healing.
Thermotherapy can be useful for helping increase blood flow to tissues when a person is unable to do warm up exercises, however, research indicates that doing warm-up exercises is more effective at increasing blood flow, oxygen and nutrient delivery than therapeutic heat so if a person is able to exercise, they should do that instead. If heat is applied for the purpose of stretching, then simultaneous stretching or stretching within 5 minutes of the treatment should occur to be therapeutically useful because there is a very short window of therapeutic effectiveness.
Summary:
Superficial thermotherapy may be useful for soothing and warming tissues, but does not do a lot beyond that. It may help reduce pain, but that also depends on the depth the heat reaches. For therapeutic ultrasound, research shows that it may be useful for soft tissue healing and repair, scar tissue, muscle spasms, trigger point areas, sympathetic nervous system disorders, fracture healing and acute inflammatory conditions (with pulsed-wave ultrasound only). Heat therapy should not occur prior to 73 hours after an injury because of negative effects from increased edema and metabolism. Depth of penetration is an important consideration in thermotherapy and thus the modality selected for treatment should be consistent with the area requiring treatment.
Sources:
Bleakley, C. M., & Costello, J. T. (2013). Do Thermal Agents Affect Range of Movement and Mechanical Properties in Soft Tissues? A Systematic Review. Archives of Physical Medicine and Rehabilitation, 94(1), 149-163.
Knight, K., & Draper, D. (2012). Therapeutic Modalities: The Art and Science [Hardcover] (p. 528). LWW; Second edition.
Robertson, V. J., & Baker, K. G. (2010). A Review of Therapeutic Ultrasound. Journal of Womenʼs Health Physical Therapy, 34(3), 99-110.
Watson, T. (2008). Ultrasound in contemporary physiotherapy practice. Ultrasonics, 48(4), 321-329.