Imagine you are living in the small residential city of Rainbow, located in Northeast Lane County, and suddenly you have a medical emergency. What if I told you the soonest you could arrive to a medical clinic would be in roughly 72 minutes? This long wait could determine life or death. In order to prevent situations of this manner in the future, research using GIScience, and spatial analysis will need to be conducted to create a plan of action to secure a better future of providing proper medical services to Lane County. In order to contribute serviceable statistics to help with these issues, future population projections and land use change models will need to be created to provide the best guidelines for proper hospital allocation for the future trends of Lane County.
The research I have conducted regarding the future growth of urban areas in Lane County will go hand in hand in order to solve the problem we are faced with, how land use changes and population increases will contribute to the increased demand on pre-existing hospital infrastructures in Lane County. Currently there are only five hospitals spread out within the entirety of the County. Will this be enough medical resources for future generations? Or will new hospitals need to be created to alleviate demand on over crowded hospitals? In order to answer this question I will conduct research on the construction of an urban area growth algorithm, in increments of five years up until the year 2030.
The meaning of the word GIS can be very open ended, and frankly I believe that the definition changes more often than not in my own dictionary. The term GIS is defined as ,“a geographic information system that allows us to visualize, question, analyze, and interpret data to understand relationships, patterns and trends”. (1.ESRI). Or in my own interpretation, a scientific system that allows for relevant and meaningful spatial analysis to be conducted in the living world that involves interpreting relationships, regions, and cultures from across the globe. So why would GIS be a good option for fixing this hospital problem? According to my research the process of using GIS for administration decision making has been increasing in the last few years.(2,pg 347). This increase in GIS and administration decision making has led to better accommodations for a growing health care reform and also for future population increases.
The use of GIScience and Spatial Analysis has been used in many other situations across the globe to attempt to predict the future populations for certain regions overtime. According to a study done in 2007, by the year 2030 60% of the worlds population will be considered an urban population.(3,pg 148). The ability to use GIS to predict the change in land use for future generations is a tool that will help lead to improving humanities ability to adapt to the increase in population and medical service demand.
This process of choosing the best suitable location for new hospital sites will be done through a series of research and analysis methods. Some of the methods of analysis that I have learned from previous projects will help with the allocation process. While I will not be assigning weights to variables to find the best suitable location for a hospital, I will still be using multiple criteria to determine the best possible placement for optimal sites. Also the standardization of all data will be key to obtaining the best possible results from the study. Because when it comes to dealing with public sector facilities such as hospitals location is key. One of the main reasons the use of location allocation analysis will be used in this study is for the purpose of maximizing accessibility for the entire Lane County community while keeping fixed and overhead costs low. I believe after these processes I believe that I will have a better answer to the main question, will future population increase projections impact the demand on the number of hospitals in Lane County, and will new hospitals need to be constructed to allow medical service access to the majority of the community?
Lane County is comprised of a unique set of forest, agricultural farmland, rural properties, and high and low density residential land type areas. The first process in this project was to decide how to categorize these land types effectively to create a small subset of land types for a more concise urban area. In order to create a land use change model of Lane county there were four different data sets that I needed to collect from places such as the “Oregon Geospatial Data Clearinghouse”, which is associated with the Oregon.gov public website . From the Oregon.gov website I collected an Oregon zoning shapefile(4.oregon.gov), which contained land types for the entire state of Oregon, however I would eventually have to create just a land zoning layer for Lane County. I also downloaded a point data-set which featured all of the large scale hospital and medical clinics in Oregon(5.oregon.gov). The last data-set which I obtained from the ESRI Street Data from the University of Oregon’s GIS Data Server.(6.ESRI) Below you can see a chart of what type of data I used and where it was obtained from.

Before I could prepare the land use data-set for the urban growth model I needed to standardize all of my data to raster form. After this process I would then set the resolution of all of the data-sets which I was working with to a standardized number. A raster data-set is essentially set up as a matrix of cells or pixels, which are organized into columns and rows. The reason why raster data is essential for this project is because each individual cell will be storing a certain value, whether this be population statistics or another land type statistic. For this project I was recommended to use a raster cell resolution of 100 acres or roughly equivalent to the size of 100 regulation sized soccer fields(7.Hazell). Because of the coordinate system being set to NAD 1983 Lambert Conformal Conic and the linear measurement being in feet the dimensions of each cell was an area of roughly 2087 ft by 2087 ft. A more informative explanation of how I achieved my urban growth algorithm can be seen below in the series of diagrams I created using Google Slides. (8. Google)
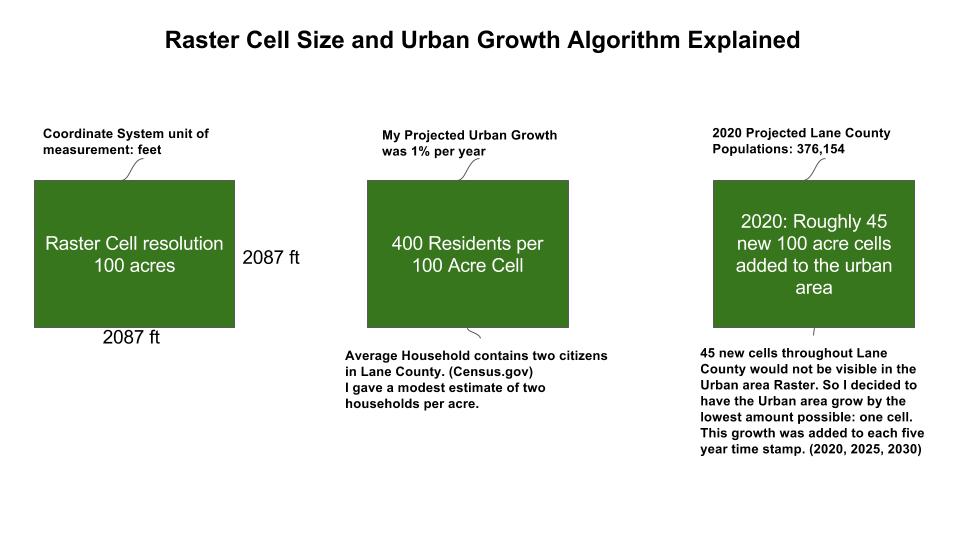
The reason I set my urban growth algorithm to only extend one cell from each urban cell per five years is because the actual growth of Lane county is projected to roughly be only 1% (9. Register-Guard). Originally I had planned on having the urban growth only to 45 new cells per five year time stamp, however this small amount of change could not be properly visualized in the ArcMap 10.3 program data view. (1.ESRI 2014). Going forward in other projects I would definitely have a smaller cell resolution to account for more accurate urban growth models.
After creating my urban growth model it was now time to prepare the data to create the three time stamps at five year intervals for future Lane County population predictions. The years for study were, 2020, 2025, and 2030, with the end result to correctly allocate new residents of Lane County to the hospitals closest to them. I have created a conceptual model of all of the steps in which I went through to correctly project future Lane County populations.

The model turned out to be very difficult to process but after several go throughs I was able to create my urban areas for the years 2020, 2025, and 2030. Processes such as conducting a euclidean distance; which is essentially computing a custom number to produce the distance which you believe the urban area will grow into in the five year period had to be computed three separate times as you can see in the above conceptual model. After the new proposed urban area had been calculated I then had to reclassify the values to equal a set value of 1, which greatly helped in the process of combining the proposed 5 year urban with the previous 2015 urban area. These steps were repeated for each of the three time stamps. Essentially the step in which I reclassified the new urban cell distance was my Urban growth algorithm for the period between 2015 and 2030.
After knowing the number of cells that were effectively new residents in Lane County I could start to convert these to demand points for the second part of the project; through location-allocation analysis. Once I created the new demand points I then used them to test the demand on each hospital location. In order to correctly determine each demand point to its corresponding hospital the network analyst tool took the network streets data-set which automatically calculated the time that it would take for each demand point to travel to each hospital. With each hospital cost distance path or time to arrive calculated, the network analyst chose the hospital location which was most suitable to each demand point. I then classified the output demand points to 5 unique categories to effectively display the demand on each location. The whole network analysis process was very intuitive and very interesting to take the ESRI Street layer(6) to conduct the location allocation analysis.
The results that I found after running the series of tests was what I expected to happen over the 15 year period. I found that the fifteen percent growth in population resulted in the expected urban expansion into many rural, forested, and agricultural based land cells. I found that the end result of the number of Urban cells grew from 624 original cells in 2015, to 2638 100 acre sized cells by the year 2030. This dramatic growth resulted in the number of park and designated green areas declining from 180 cells in 2015 to just 69 by the year 2030, that is a 62% overall loss for these green areas. If I were to go back and redo this project I believe that I would have reclassified the green areas as areas of constraint, or areas which urban growth was inhibited to expand into. This is because I assume by the year 2030 society will surely be managing green spaces and parks with the same recognition as of today’s standards. After my results of my urban growth algorithm I found that the urban areas had expanded well within the designated forest and agriculture lands. In 2015 the number of cells designated as forest or agriculture lands was as high as 28,492 100 acre cells or roughly 97% of the total area of Lane County. In the first 5 year time stamp; year 2020, the number had declined to 27,987 total cells or roughly 95% of total area. I was a little confused by this small percentage of change, however if you change the scale on the amount of land converted to urban areas then the number is around 95 square miles throughout Lane County. By the year 2025 the number of square miles lost to urban areas was up to 189 square miles or 4% forest and agriculture loss from the 2015 total. At the end of the last time stamp in 2030 the lost forest and agriculture areas was up to a total of 6% or 283 square miles throughout Lane County. In my map of Urban Expansion in the 15 year period you can see the amount of land change first hand.

Respectively you can compare the two maps with each other, regarding the land cover change over the 15 year period.

In the fifteen year period of urban growth, I had predicted a population growth of 1% per year, and over the fifteen years this number compounded to equal 56,373 new residents in Lane County. By my previous urban growth algorithm where I assumed that the growth of the county would not warrant a tremendous amount of new cells, I found out that if you take the 56,373 new residents and divide that between the 2,014 number of new urban cells then you would have roughly only 28 residents living in a 100 acre area. But because of the nature of such a large cell size, I decided to adopt the least possible cell growth for each of the three five year time stamps to at least show a slight visual change. This adoption of a larger urban growth algorithm and raster cell size would definitely be better implemented in a higher densely populated county such as Multnomah County.
Present day Lane County has some issues regarding its low number of large scale hospitals. With the results that I have found in this research the number of patients per hospital could become a major issue in the near future. This population growth adds stress to the road systems across Lane County which will contribute to longer time periods to reach a potential hospital. As I mentioned in the beginning of my journal, some locations in Lane County have as much as a 72 minute drive to the nearest hospital location. With the increase in residents comes the need for better road infrastructure and new hospital development to alleviate stress from over crowded hospitals. The results I found for present day hospital demand was a little astonishing. With only five major hospitals in Lane County the number of patients per hospital is a definite issue. The Sacred Heart University District Medical Center alone has to provide services for 39% of the Lane County population. More figures and maps on Lane County Hospital Allocation over the 15 year time period can be seen below.




Because of a high population increase in cities such as Veneta; west of Eugene, and Junction City; Northwest of Eugene by the year 2030 I decided that a suitable location for a proposed hospital would be most beneficial in the area in the middle of each three. Using both the network streets layer,and Google Earth (10.Google), I found a suitable site in west Eugene located on west 11th ave. I found a sizable area of undeveloped land to allocate for the proposed hospital site. Below you can see how the stress on the University District Sacred Heart medical Center has been lessened by this new medical clinic.


As you can see the new hospital immediately helps the demand percentage of the University District hospital. The demand on the sacred Heart hospital drops from the original 39% to just 18% of the total population. However I was not done proposing new hospital sites, through the same process as the west 11th ave location I found another suitable location in east Springfield off of highway 126. I chose this location because the urban areas near this location had grown a great amount during the 15 year period. I also took into account the fact that McKenzie-Willamette Medical Center was receiving 29% of the patients throughout Lane County. With the introduction of the new hospital in eastern Springfield this dropped the demand on the McKenzie-Willamette center to less than 10%. Below you can see in the map and chart I created the new demand on the five Lane County hospitals when combined with two proposed hospital sites.


When comparing the various maps and diagrams after finishing my analysis portion of the project, I realized that perhaps the best thing to come out of this project was the awareness. The awareness that Lane County and on a smaller scale the city of Eugene is no where close to having the correct ratio between patients and number of hospitals. I believe that through processes such as location allocation, and urban growth models we can develop plans of action to find suitable sites for new potential hospitals. These new hospitals would help alleviate stress from the five current hospitals that are trying to stay sustainable presently. Alternatively these same spatial analysis processes can be used on larger scales in global projects.These projects could include allocating disaster relief stations near areas where earthquake and tsunami hazard zones are the greatest, or by providing health clinics to third world and developing countries where they are needed the most.
When I encountered errors when conducting the analysis portion of this project they were not really in the manner of vagueness or discrepancies in the data-sets, but rather problems in properly defining the measurement of attributes and measurements of space for my data.(11. Fisher) These errors can mostly be associated once again with the large raster cell resolution classified in the beginning of the project. Other errors I encountered were mostly software based such as attempting to combine and overlay the various raster data sets that were used in the analysis. I had trouble with my ArcMap program (1) in the fact that it kept crashing every time I would try to overlay the new urban area with the original land use raster layer. However to combat this error I developed a different model or workflow which in the end led to some discrepancies in my end results. Because of this overlay issue I was not able to keep the urban areas from expanding into such cells as the water bodies, and green areas and parks. If I were to go back and reproduce this project I would definitely create an alternative way to keep the urban areas from developing into what is the Fern Ridge Reservoir. Alternatively I will reiterate that a smaller resolution would be a better option for future projects in this same manner, as it would allow for a finer urban growth algorithm, and more accurate land use change models. I believe in order to use such a large cell size (100 acres) you would want to focus your attention to a larger county with a higher population density. With these larger cell sizes you lose accuracy when attempting to find a suitable new location for a medical clinic.
In future projects when dealing with land use change, and medical service allocation, I believe I would add a step towards the end of my analysis. I would implement a Multi-Criteria Evaluation to determine what area of the future projected landscape would be most suitable for the new hospitals. I would choose a few variables to analyze and based off of those results I would be able to choose a more suitable location, rather than just relying on the network streets data, and Google Earth. Some possible criteria could be soil data, household income data, and average household age data. This Multi-Criteria approach as the last step is very important in determining the best location based on temporal and financial constraints which might hinder the addition of a new medical clinic in some zones of the county.(12.pg 157).
While I would not go as far as saying future Lane County population projections are significant, I would say that even in 2015 the high ratio between patients and hospital allocation is a critical issue, and will continue until more medical service centers are provided.
[1] ESRI 2014. ArcGIS Desktop: Release 10.3.1. Redlands, CA: Environmental Systems Research Institute.
[2] Taylor, Devon M. et al.. “USING GIS FOR ADMINISTRATIVE DECISION-MAKING IN A LOCAL PUBLIC HEALTH SETTING”. Public Health Reports (1974-) 127.3 (2012): 347–353. Web…
[3] Liu, Xiaoping, et al. “Simulating Urban Growth By Integrating Landscape Expansion Index (LEI) And Cellular Automata.” International Journal Of Geographical Information Science 28.1 (2014): 148-163. Academic Search Premier. Web. 6 Dec. 2015.
[4]Oregon Zoning Shapefile. N.p.: Oregon Geospatial Data Clearinghouse, n.d. .zip.http://www.oregon.gov/DAS/pages/irmd/geo/sdlibrary.aspx
[5]Oregon Hospital Point Feature Data. N.p.: Oregon Geospatial Data Clearinghouse, n.d. .zip.http://www.oregon.gov/DAS/pages/irmd/geo/sdlibrary.aspx
[6]Network Street Data. N.p.: ESRI, University of Oregon GIS Database, n.d.
[7]Hazell, Alastair. “How Big Is An Acre? Explained.” The Calculator Site, n.d. Web. 05 Dec. 2015.
[8]Google Inc. (2009). Google Slides [Software]. Available from
https://www.google.com/docs/about/
[9] Hubbard, Saul. “Oregon’s Population Hits 4 Million.” The Register-Guard, 18 Nov. 2015. Web. 03 Dec.
[10]Google Inc. (2009). Google Earth (Version 5.1.3533.1731) [Software]. Available from
https://www.google.com/earth/
[11]Fisher P F. Models of Uncertainty in Spatial Data. pgs: 196–197
[12]Malczewski, J., and Ogryczak, W., 1990, An interactive approach to the central facility location problem: locating pediatric hospitals in Warsaw. Geographical Analysis, 22, 244–258.
“Maps throughout this journal were created using ArcGIS® software by Esri. ArcGIS® and ArcMap™ are the intellectual property of Esri and are used herein under an academic license. Copyright © Esri. All rights reserved. For more information about Esri® software, please visit www.esri.com.”